Cranial Neuralgias

Cranial Neuralgias are structural and/or functional abnormalities in the central nervous system and peripheral nervous system. They may be caused by infection, trauma, chemotherapy/radiation, surgery, neurotoxins, compression, inflammation, or tumor irritation. Oftentimes patients describe an electric shock like or lancinating pain and almost always has a unilateral presentation. There are two broad categories of cranial neuralgias: episodic or continuous symptoms.
|
Those with episodic symptoms:
Typically lasts seconds to minutes and may either be frequent or separated by long periods of remission. Often occurs following a triggering event such as a superficial, delicate touch of face or mouth. |
Those with continuous symptoms:
Typically presents with a varying intensity of dull aching, burning, or throbbing with bouts of sharp pain. Patients with continuous symptoms have no total remission and is often mistaken mistaken as a toothache or headache. |
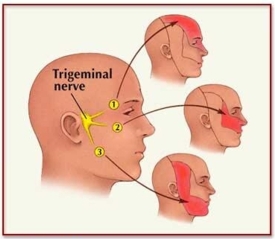
Trigeminal Neuralgia
Trigeminal neuralgia (TN), classified as an episodic paroxsymal pain, is the most common form of cranial neuralgia, with 4.3 cases per 100,000 persons each year. It affects women more than men. Trigeminal neuralgia occurs when there is compression of the trigeminal nerve, pictured to the right, near the brainstem. This leads to a mechanical twisting of the fibers and secondary dymyelination of the fibers.
|
Presentation
Usually affects the 2nd or 3rd division of the nerve and on one side of the face. The right side more commonly affected than the left. Patients complain of a sudden onset of sharp, stabbing pain which can last less than a second to a few seconds. Occasionally they'll present as a cluster of variable intensity lasting up to 2 minutes each. The trigger may be a light touch on the skin, eating, shaving, washing, applying makeup, brushing of the teeth, movement of the jaw or tongue, or a thermal stimulus. Recurrence is common |
http://www.nanovibronix.com/Nano/UpLoadFiles/PGallery/2911668347.jpg
|
|
ICHD-3 Diagnostic Classifications:
At least three attacks of unilateral facial pain fulfilling the next two criteria Occurring in one or more divisions of the trigeminal nerve, with no radiation beyond the trigeminal distribution Pain has at least three of the following four characteristics:
No clinically evident neurologic deficit Not better accounted for by another ICHD-3 diagnosis |
|
|
Recommendations
Call to the physician, especially if undiagnosed, and treat the patient.
|
Differential Diagnosis
|
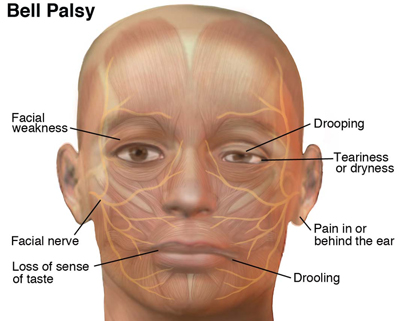
Bell's Palsy
Bell's Palsy is an acute peripheral facial palsy of unknown causes and affects the branches of the facial nerves. Bell's Palsy represents half of all facial palsies with between 13-34 cases per 100,000 persons. The prognosis is related to the severity of the lesion. There are many theories or beliefs as to what leads to Bell's Palsy. One of which is the belief that the herpes simplex virus may be the cause but this has proven difficult to test in most cases. Herpes Zoster is estimated to be the second most common cause. Finally, when occurring in pregnancy, it is believed that the fluid-retention found in pregnancy leads to compression of the facial nerve.
|
Presentation
Patients often display an increased psychological stress secondary to the facial palsy. Remember: Sparing of the forehead is indicative of a central lesion |
http://www.moveforwardpt.com/
|
|
Diagnosis
The diagnostic criteria include:
To diagnose, a neural examination of Cranial Nerve VII should be performed. To see an example of this test, see the video to the right. |
|
|
Differential Diagnosis
|
Risk Factors
The risk is 3 times greater during pregnancy, especially in the third trimester or in the first postpartum week. Red Flag: History of a facial twitch or spasm that precedes the facial weakness suggests nerve irritation from a tumor and should prompt referral and further imaging.
|
Recommendations
Call to the patient's physician and treat the patient
|
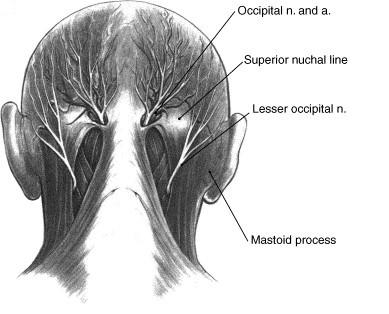
Occipital Neuralgia
Occipital neuralgia can be the cause of headache-type pain in the occipital region. The condition is considered rare; however, the literature is conflicting. Overall, the actual incidence and prevalence are unknown.
|
Presentation
Risk Factors
Whiplash types of injuries in MVAs may increase your chance of an occipital neuralgia |
http://drlox.com/images/stories/images/occipital%20nerves.jpg
|
|
Diagnosis
Overall, there lacks a consensus on the specific diagnostic criteria for occipital neuralgia. Often any occipital pain is arbitrarily called "occipital neuralgia" and referred to a specialist. Requires a careful examination of the upper cervical spine and occipital regions. Recommendations
Call to physician and treat the patient
|
Differential Diagnosis
|
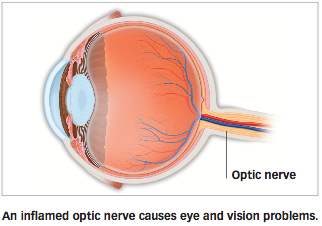
Optic Neuritis
Optic neuritis is an inflammatory, demyelinating condition which affects a single eye. Eventually this will cause vision loss. This is a common presentation of multiple sclerosis (MS) and may require you to refer out if your patient is undiagnosed but expect this as the underlying cause. Optic neuritis has an incidence of roughly 6 cases per 100,00 persons in the United States, with it more common in women than men.
|
Presentation
|
http://www.allaboutaesthetics.com/_media/img_eye_facts/optic-neuritis.png
|
|
Diagnosis
A full opthalmologic examination is highly recommended if optic neuritis is suspected. Pupillary Defect
|
|
|
Differential Diagnosis
|
Recommendations
Refer to a physician. Remember to assure the patient that in most cases, near full recovery of vision occurs. |
Herpes Zoster
Herpes Zoster, or more commonly known as shingles, is a continuous neuropathic pain. It occurs after a previous varicella or chickenpox infections as it moves into the dorsal root and cranial nerve ganglia for a period of dormancy. Typically, this latency is lifelong but for some, an outbreak of shingles occurs. In healthy individuals, the recurrence is uncommon but recurrence is common in the immunocompromised population.
|
Presentation
Rash: the key presentation in shingles. The rash is seen as a group of vesicles occurring across a single dermatome. Occasionally the rash will affect the surrounding dermatomes.
Systemic System
Herpes Zoster Opthalmicus
|

Herpes Zoster rash from UpToDate
Diagnosis
A unilateral vesicular eruption in a well-defined dermatomal pattern as seen in the picture above. Requires a viral culture to confirm
|
|
Differential Diagnosis
|
Risk Factors
immunocompromised (HIV / AIDs) |
Recommendations
Refer to the patient's primary care physician and encourage the patient to engage in physical activity as tolerated. If the patient is seen in the hospital or rehab setting, it may be necessary to protect the skin with dry dressings. |
