Trauma
Whiplash

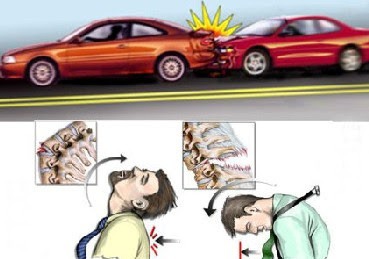
Cervical hyperextension injuries, often referred to as 'whiplash' injuries, are caused most commonly by motor vehicle accidents, but such injuries also can occur in contact sports, from falls (either at ground level or from height), or by being struck on the head by a falling object.
Cervical hyperextension injuries typically occur in seated occupants of a stationary or slow-moving vehicle that is struck from behind. The body is thrown forward, but the head lags due to inertia, resulting in hyperextension of the neck. When the head and neck have reached maximum extension, the neck snaps into flexion. Automobile headrests play a major role in preventing or reducing the severity of these injuries. Cervical hyperextension injury also should be considered in patients presenting with significant facial trauma after a fall.
Typical clinical findings include neck pain, paraspinal muscle tightness, and spasm. Neck pain develops shortly after the inciting event and may worsen and peak 24 to 48 hours later. Injury to the muscle can cause bleeding, swelling, muscle spasm, and pain
Headaches develop in many patients, and head injury should be excluded, particularly in patients with significant facial trauma. Symptoms can last weeks to months; 20% to 40% of patients develop chronic symptoms. Symptoms such as leg weakness, hyperactive tendon reflexes in the legs, upgoing plantar response, and/or sphincter disturbance suggest damage to the spinal cord. Arm weakness or numbness suggests damage to the nerve roots of the cervical spine. Neurologic deficits are rare, unless an accompanying cervical spine fracture or central cord syndrome is present.
Cervical hyperextension injuries typically occur in seated occupants of a stationary or slow-moving vehicle that is struck from behind. The body is thrown forward, but the head lags due to inertia, resulting in hyperextension of the neck. When the head and neck have reached maximum extension, the neck snaps into flexion. Automobile headrests play a major role in preventing or reducing the severity of these injuries. Cervical hyperextension injury also should be considered in patients presenting with significant facial trauma after a fall.
Typical clinical findings include neck pain, paraspinal muscle tightness, and spasm. Neck pain develops shortly after the inciting event and may worsen and peak 24 to 48 hours later. Injury to the muscle can cause bleeding, swelling, muscle spasm, and pain
Headaches develop in many patients, and head injury should be excluded, particularly in patients with significant facial trauma. Symptoms can last weeks to months; 20% to 40% of patients develop chronic symptoms. Symptoms such as leg weakness, hyperactive tendon reflexes in the legs, upgoing plantar response, and/or sphincter disturbance suggest damage to the spinal cord. Arm weakness or numbness suggests damage to the nerve roots of the cervical spine. Neurologic deficits are rare, unless an accompanying cervical spine fracture or central cord syndrome is present.
|
Causes:
|
Risk Factors:
|
|
Symptoms:
|
Signs:
|
Other Historical Factors:
|
|
Physical Examination:
|
Diagnostic Testing:
|
Treatment:
- High-dose methylprednisolone administered within 8 hours of injury, with the aim to reduce edema and its effects on the spinal cord as soon as possible, may be beneficial in patients with acute spinal cord injury. However, use of high-dose corticosteroids in the setting of spinal cord injury is controversial, and several studies suggest that the risks and disadvantages may outweigh the potential benefits; hence, many institutions are moving away from this practice Use of ice packs within the first 24 hours and moist heat thereafter is a general recommendation for soft tissue injuries
- Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen and naproxen , or acetaminophen , often in conjunction with manual therapies, may be used in patients with mild injuries. Muscle relaxants, such as cyclobenzaprine , also may be useful, as they reduce muscle tightness and spasms, thereby improving mobility and pain. The majority of cervical hyperextension injuries that involve only the soft tissues will resolve with the use of NSAIDs and muscle relaxants in a matter of weeks
- Soft cervical collars give useful support to an injured neck but should be used for no more than 2 weeks
- Use of a cervical spine pillow cradles the head and supports the neck may be advisable
Physical Therapy Implications (Recommendations):
- The goals of management of patients with cervical hyperextension injuries are to exclude serious injury to nerve roots, the spinal cord, and vertebrae; resolve symptoms; improve the patient's functional status and lessen the need for time off from work; and reduce long-term disability
- Manual therapies, such as active physical therapy exercises and spinal manipulations, are helpful in many patients who are at extremely low risk. Active physiotherapy should not be initiated until it is clear that the spinal cord is not at risk of compromise and the cervical spine is stable. Spinal manipulation is contraindicated in patients with spinal injuries
- Lifestyle changes, including early resumption of normal activity, should be considered
Concusions

Concussion is caused by a direct blow to the head, face, neck, or other
body area with an 'impulsive' force transmitted to the head, resulting in a
rapid acceleration, deceleration, or rotation of the brain, and is classified
as a functional disturbance rather than a structural injury
Features include rapid onset of short-lived impairment of neurologic function that resolves spontaneously, a graded set of clinical symptoms that may or may not involve loss of consciousness and may be prolonged in a small percentage of patients, and absence of abnormalities on standard structural neuroimaging studies
Features include rapid onset of short-lived impairment of neurologic function that resolves spontaneously, a graded set of clinical symptoms that may or may not involve loss of consciousness and may be prolonged in a small percentage of patients, and absence of abnormalities on standard structural neuroimaging studies
|
Epidemiology:
|
Causes:
Risk Factors:
|
Screening:
For athletes participating in contact and collision sports, preseason baseline postural stability testing ( eg , Balance Error Scoring System) and neuropsychological testing, including computerized tools and brief test batteries, such as the Standardized Assessment of Concussion and Sport Concussion Assessment Tool 2, are important tools that provide an individualized assessment of an athlete's balance and cognitive function; such tests also are of value in providing a baseline against which to compare performance, as an on-site tool in assessing the possibility of concussion in the event of injury, and to serially monitor recovery from concussion.
For athletes participating in contact and collision sports, preseason baseline postural stability testing ( eg , Balance Error Scoring System) and neuropsychological testing, including computerized tools and brief test batteries, such as the Standardized Assessment of Concussion and Sport Concussion Assessment Tool 2, are important tools that provide an individualized assessment of an athlete's balance and cognitive function; such tests also are of value in providing a baseline against which to compare performance, as an on-site tool in assessing the possibility of concussion in the event of injury, and to serially monitor recovery from concussion.
|
Symptoms:
Clinical Symptoms can fall into one of four categories: 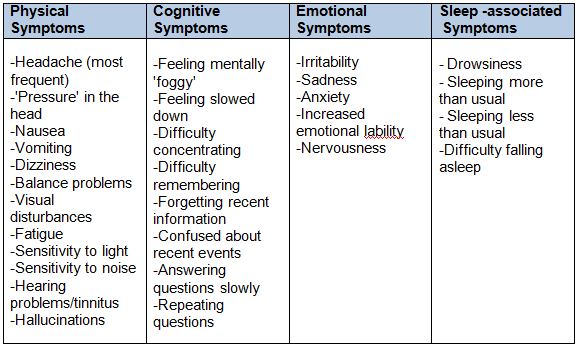
|
Signs:
|
|
Differential Diagnosis:
|
|
Physical Therapy Implications (Recommendations):
Refer out if:
|
